✍️ Written by: LSRI Editorial Team
🩺 Medically Reviewed by: Dr Prashant Sankaye, Consultant Musculoskeletal specialist and Radiologist, MBBS, MS, FCPS, MRCS, CCBST, FRCR, PGCE(Med), FHEA, PGDip Sports and Exercise Medicine
📅 Last Updated: April 17, 2026
⏱️ Read Time: 16 Minutes
By Dr Prashant Sankaye FRCR, Consultant Musculoskeletal, Spine & Sports Radiologist | LSRI & Scannearme
Last medically reviewed: April 2026 by Dr Prashant Sankaye FRCR, Consultant Musculoskeletal, Spine & Sports Radiologist This is a clear example of how delayed diagnosis stress fractures can impact patient outcomes.
“Diagnosis shouldn’t be a question of luck.” That was the message from Health Secretary Wes Streeting in April 2026 as he announced £237 million of new government investment in Community Diagnostic Centres across England, calling it the biggest expansion of NHS diagnostics in a generation. He spoke from personal experience — his own kidney cancer was caught early, and he is now cancer-free. He acknowledged plainly that not every patient is so fortunate. This is a clear example of how delayed diagnosis stress fractures can impact patient outcomes.
That message resonates deeply with what I see in my daily clinical practice as a musculoskeletal and sports radiologist specializing in the delayed diagnosis of stress fractures. Whether the problem is cancer or a bone stress injury, the single most preventable harm in medicine is a delayed diagnosis — one that allows a treatable problem to become a devastating one while a patient is reassured, passed between services or simply told to “wait and see”. This is a clear example of how delayed diagnosis stress fractures can impact patient outcomes.
This article is about one such case, and about the wider principle it represents. It is also about what patients, GPs, physiotherapists and the wider NHS can do differently — starting today.
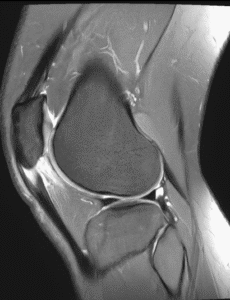
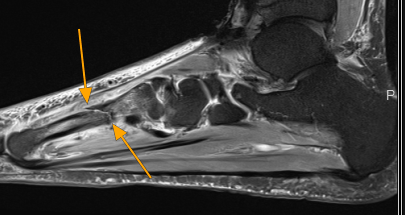
Delayed Diagnosis Stress Fractures: What you are looking at in these MRI images

The four-panel MRI above is not unusual. What is unusual — and deeply concerning — is the story behind it.
This patient came to me after eight months of persistent foot pain. Eight months during which they attended their GP. Eight months during which they were referred to physiotherapy. Eight months in which they were reassured, treated for “soft-tissue injury” and asked to keep going. And then the bone broke. This is a clear example of how delayed diagnosis stress fractures can impact patient outcomes.
What the MRI shows is a complete metatarsal stress fracture — bright signal flooding the surrounding bone marrow on the fluid-sensitive sequences (lower panels), a clear low-signal fracture line visible on both the sagittal (top-left) and coronal planes, and the orange arrows pointing to the site of failure that has now progressed from a stress reaction to a full cortical break. This is a clear example of how delayed diagnosis stress fractures can impact patient outcomes.
At the stress-reaction stage — weeks or months earlier — the X-rays were almost certainly normal. The physiotherapy referral was made in good faith. The GP was working within the constraints of a system that does not always make MRI easy to access. But the outcome was still preventable. This is a clear example of how delayed diagnosis stress fractures can impact patient outcomes.
Understanding bone stress injuries — a spectrum, not a single event
Bone stress injuries do not happen suddenly. They develop along a continuum, from the earliest invisible changes to complete fracture.
| Stage | What is happening in the bone | What imaging shows | Risk if ignored |
|---|---|---|---|
| Stress reaction (Grade 1–2) | Microfractures and bone marrow oedema; cortex intact | Normal or near-normal X-ray; MRI shows marrow signal change only | Fully reversible with rest and load management — recovery typically 6–8 weeks |
| Stress fracture (Grade 3) | Visible fracture line; bone marrow oedema; cortex disrupted but not fully broken | Faint or subtle X-ray change (easily missed); MRI shows clear fracture line + oedema | High risk of complete fracture if loading continues |
| Complete fracture (Grade 4) | Full-thickness cortical break; possible displacement | Clear on X-ray; extensive changes on MRI | Immobilisation, possible surgery, prolonged recovery, risk of non-union |
The critical insight here is that early diagnosis at Grade 1–2 is almost always curative with conservative management alone. Every week of delay beyond that point moves the patient closer to a Grade 3 or 4 injury — with exponentially greater consequences for their health, their livelihood and the NHS resources required to treat them. This is a clear example of how delayed diagnosis stress fractures can impact patient outcomes.
Why stress fractures are so frequently missed
This is not a question of negligence in most cases. It is a question of systems, incentives and access to the right tools at the right time.
X-rays are almost always normal in the early stages
Plain X-ray — the first test most patients receive — has a sensitivity for stress fractures of only 12–56% in published studies. This means that up to 88% of early stress fractures are simply invisible on X-ray. Subtle periosteal reaction, when it does appear, is easy to overlook and may only develop weeks after symptoms begin. This is a clear example of how delayed diagnosis stress fractures can impact patient outcomes.
A patient presenting with foot or shin pain, a normal X-ray and no obvious trauma will frequently be labelled as having soft-tissue injury — not because the clinician has failed, but because the test being used cannot detect what is actually wrong. This is a clear example of how delayed diagnosis stress fractures can impact patient outcomes.
MRI is the gold standard — but access is not equal
MRI has sensitivity of 68–99% and specificity of up to 97% for stress fractures of the lower extremity. It is the only investigation that can detect bone marrow oedema before any fracture line has developed, giving a genuine window of opportunity to intervene early. This is a clear example of how delayed diagnosis stress fractures can impact patient outcomes.
Yet same-week or even same-month MRI access is far from universal in the NHS, particularly for non-urgent, non-elite patients with foot or shin pain. The Community Diagnostic Centre expansion announced by Wes Streeting is designed precisely to address this kind of diagnostic bottleneck — but until that infrastructure is in place, patients face a choice between waiting and going without answers.
Physiotherapy without a diagnosis is a gamble
Physiotherapy is a valuable profession and physiotherapists provide excellent care. But soft-tissue rehabilitation applied to an undiagnosed bone stress injury does not help — and continued loading of a weakening bone actively accelerates the path to complete fracture.
The problem is not physiotherapy itself. The problem is treating before diagnosing. When the diagnosis is wrong, the treatment — however skilled — cannot be right.
High-risk fracture sites need urgent imaging regardless of X-ray result
Some anatomical locations carry a disproportionate risk of serious complication if missed — including the femoral neck, anterior tibia, tarsal navicular, and fifth metatarsal base. At these sites, a stress fracture can progress to complete fracture, avascular necrosis or non-union with devastating functional consequences. Updated guidance from the American College of Radiology emphasises that early advanced imaging is recommended for high-risk sites even when X-rays are negative.
What can go wrong — and what has gone wrong
The medico-legal record in the UK makes sobering reading:
- A patient received £40,000 compensation after a stress fracture was not correctly identified, progressing to an avoidable complete femoral fracture requiring surgical intervention.
- Legal action has been taken in cases where clinicians failed to recognise red-flag features, did not arrange appropriate imaging, or mis-reported imaging, with patients sustaining major fractures as a direct result.
- An NHS Trust faced litigation after a tibial stress fracture evolved into a complete cortical fracture due to delayed diagnosis and treatment, confirmed retrospectively on MRI.
These are not isolated incidents. A 2025 international patient safety study from Imperial College London found that the UK is not improving patient safety outcomes as quickly as comparable health systems, despite clinical expertise and technologies for earlier diagnosis already being available.
The NHS Safety Investigation Body has separately documented how failures in clinical communication — including discharge summaries not reaching GPs — have led to direct patient harm when diagnoses were not followed up.
In each of these cases, the final outcome was worse than it needed to be. The bone broke, the cancer progressed, the treatment window closed. And in almost every case, earlier imaging would have changed the story.
The national context — diagnosis as a patient right, not a privilege
When Wes Streeting announced the £237 million CDC investment in April 2026, he framed it as a moral imperative — not just an NHS efficiency measure.
“The NHS should be there for all of us when we need it, catching illness earlier so we can treat it faster. Community Diagnostic Centres mean patients can get tests, checks and scans while they’re doing their shopping at the weekend or on the way to pick up the kids from school — without travelling across town to a hospital.”
The new CDCs — four new sites opening in Gorton, Luton, Boston and Bideford in 2026/27, plus 17 expansions — are part of a wider drive to close the gap between patients who get early diagnoses and those who do not.
This policy direction matters deeply for musculoskeletal patients. CDCs that offer MRI and ultrasound in community settings could make early bone stress injury diagnosis far more accessible — but only if GPs, physiotherapists and sports clinicians know when to refer for imaging, and only if patients know they have the right to ask.
The wider picture — delayed diagnosis in cancer
The same principles that apply to a metatarsal stress fracture apply, with even higher stakes, to cancer.
Over one in three patients referred by their GP with suspected cancer are now waiting longer than the 28-day diagnostic standard in England. Research modelling shows that a four-week delay in cancer diagnosis can increase the risk of death by approximately 10% for common cancers. For lung cancer, a six-week diagnostic delay has been associated with a drop in five-year survival from 61% to 38%.
The costs of diagnostic delay in cancer were starkly quantified during the COVID-19 pandemic, when LSHTM modelling predicted that diagnostic delays could result in an additional 3,300–3,500 breast and bowel cancer deaths over five years — equivalent to almost 60,000–63,000 years of life lost.
These statistics are not abstract. They represent individual patients whose cancer was treatable at Stage 1 and became terminal by Stage 3. Just as a stress fracture that could have been managed conservatively becomes a surgical emergency if ignored, a cancer diagnosed at Stage 1 is a fundamentally different illness to one diagnosed at Stage 4.
The unifying principle is simple: every day of diagnostic delay has a price.
What “diagnose first, treat later” means in practice
At LSRI (London Sports and Rheumatology Imaging) and through Scannearme, my ethos is built on a single conviction: you cannot treat what you have not accurately diagnosed.
This means:
- Taking a thorough clinical history — training load, symptom timeline, previous treatment, risk factors for bone fragility — before deciding what investigation is needed.
- Choosing the right imaging modality for the clinical question. For suspected bone stress injury, that is almost always MRI first, not X-ray first.
- Not accepting a normal X-ray as sufficient reassurance when the clinical story points towards bone stress injury, particularly at high-risk sites or after weeks of persistent, localised, load-related pain.
- Correlating imaging findings with clinical context — a Grade 2 stress reaction found at the right moment allows conservative management; a Grade 4 complete fracture found eight months later requires immobilisation and potentially surgery.
- Communicating clearly and promptly — both to the patient and to the referring clinician — so that the right protective measures are in place before the next training session, not after the next fracture.
This is not a radical idea. It is what evidence-based MSK medicine looks like when it is working properly.
When should patients push for imaging — red flags for bone stress injury
Patients should not need to fight for appropriate imaging. But in a system under pressure, knowledge is power. The following should prompt a direct conversation about whether MRI is indicated:
- Localised bone tenderness on a specific point of a bone — not vague, diffuse muscle ache, but a sharp, exact point that hurts when pressed.
- Pain that worsens reliably with activity and eases with complete rest, especially if this pattern has persisted for more than 4–6 weeks despite appropriate conservative measures.
- Pain that has started appearing at rest or at night — this suggests the injury is progressing beyond a simple stress reaction.
- Inability to hop or single-leg balance on the affected limb without significant pain.
- A clear precipitating change — new sport, sudden increase in training volume, change of surface, new footwear, return from injury.
- High-risk location — femoral neck, anterior tibial cortex, tarsal navicular, fifth metatarsal base, sesamoids.
- Risk factors for poor bone health — post-menopausal status, known osteoporosis, low vitamin D, disordered eating, menstrual disturbance in female athletes (the female athlete triad or RED-S).
If three or more of these are present, waiting for an X-ray result before arranging MRI is unlikely to be helpful and may cause avoidable harm.
How LSRI supports accurate, early diagnosis
LSRI — London Sports and Rheumatology Imaging — exists to provide consultant-led, specialist musculoskeletal imaging with the full weight of expert clinical correlation, not just image reporting as a routine service.
As the lead consultant radiologist, I bring specific expertise in:
- Sports injuries and bone stress imaging — grading stress reactions accurately, identifying high-risk fracture patterns, and helping clinicians make safe return-to-sport decisions.
- Complex spinal imaging — including lumbar pars stress injuries, disc pathology and facet joint disease in athletic and non-athletic patients.
- Rheumatological and inflammatory conditions — where MRI and ultrasound are essential to distinguishing inflammatory joint disease from mechanical injury.
- Ultrasound-guided procedures — where needed, guided injections and aspirations using real-time imaging to ensure precision.
LSRI works closely with orthopaedic surgeons, rheumatologists, sports medicine physicians and physiotherapists, so that a diagnosis leads directly to action rather than sitting in a queue.
How Scannearme makes fast, expert MRI accessible across the UK
For patients outside London, or for those facing long NHS waiting times, Scannearme (scannearme.co.uk) provides a practical route to affordable, high-quality MRI across a national network of partner centres.
Key features:
- UK-wide coverage — partner MRI centres across England, Scotland and Wales, with appointments often available within days.
- Transparent, affordable pricing — clear costs upfront, without the need to navigate complex insurance or referral pathways.
- Self-referral supported — patients can initiate a booking with clinical triage to ensure the right scan is requested safely and appropriately.
- Expert reporting — reports from radiologists with appropriate specialist experience, with MSK and sports imaging expertise available for complex bone stress cases.
- Digital delivery — images and reports delivered directly to you and to your chosen clinician, whether NHS or private, supporting continuity of care.
For a runner with eight weeks of shin pain and a normal GP X-ray, Scannearme can provide a same-week MRI at a nearby centre, an expert report within 24–48 hours, and clear guidance on whether the injury is a stress reaction that needs rest or a stress fracture that needs urgent orthopaedic review.
That is the difference between diagnosis at Grade 2 and presentation with a complete fracture at Grade 4.
A message to GPs, physiotherapists and sports clinicians
This article is not a criticism of primary care or physiotherapy. Both are essential, and in the vast majority of musculoskeletal presentations, clinical assessment and initial conservative management are exactly right.
But when persistent, localised bone pain is not resolving as expected — especially in active patients, in post-menopausal women, in patients with RED-S risk factors, or at anatomically high-risk sites — the question “could this be a bone stress injury?” deserves an MRI answer, not a further four weeks of physiotherapy.
The evidence is clear: X-ray misses the majority of early stress fractures. MRI detects them with sensitivity and specificity that no other widely available modality matches. The cost of an early MRI — financial, clinical and human — is a fraction of the cost of treating a complete fracture, a surgical repair, or a protracted period of non-weight-bearing rehabilitation.
Early referral is not over-investigation. In this context, it is good medicine.
FAQs — Delayed diagnosis, stress fractures and early MRI
Why does a stress fracture not show up on X-ray?
Plain X-rays detect cortical disruption and bony changes — they are poorly suited to detecting the early bone marrow oedema and microdamage that characterises a stress reaction or early stress fracture. Studies show X-ray sensitivity for stress fractures as low as 12–56%, meaning most early stress fractures are simply invisible. MRI detects the same injuries with sensitivity of up to 99%.
How long is too long to wait before requesting an MRI for foot or shin pain?
If localised, activity-related bone pain has not resolved after 4–6 weeks of appropriate rest and activity modification, MRI should be strongly considered — particularly if any red-flag features are present. Waiting longer risks allowing a reversible stress reaction to progress to a complete fracture.
What is a “high-risk” stress fracture and why does it matter?
High-risk stress fractures occur at sites prone to non-union, displacement or avascular necrosis if missed — including the femoral neck, anterior tibia, tarsal navicular, fifth metatarsal base and hallux sesamoids. At these sites, current guidelines recommend early MRI even with a normal X-ray because the consequences of delay are severe.
What does Dr Prashant Sankaye mean by “diagnose first, treat later”?
It means that targeted, expert imaging must precede treatment decisions whenever persistent or escalating pain is not explained by clinical examination alone. Treating on assumption rather than diagnosis risks months of misdirected management — as illustrated by the case in this article, where eight months of treatment for “soft-tissue injury” allowed a metatarsal stress fracture to progress to complete bone failure.
How can I access an MRI scan quickly through Scannearme?
Visit scannearme.co.uk to find your nearest partner MRI centre, check available appointment slots and transparent pricing, and complete a brief clinical triage. Reports are delivered digitally and can be shared with your GP, physio, orthopaedic surgeon or rheumatologist. No hospital referral is required for most MSK scans.
What is LSRI and how is it different from a general radiology department?
LSRI — London Sports and Rheumatology Imaging — is a specialist MSK imaging service led by Dr Prashant Sankaye FRCR, combining subspecialty expertise in sports injuries, bone stress pathology, spinal imaging and rheumatological conditions with close integration with referring clinicians. This means images are reported with full clinical correlation and context, not as an isolated administrative task.
References and further reading
- Wes Streeting, April 2026 — “Diagnosis shouldn’t be a question of luck”: Yahoo News | Independent
- StatPearls: Stress Reaction and Fractures — National Institutes of Health: NIH/StatPearls
- Mandell et al., American Journal of Roentgenology — Diagnostic accuracy of imaging modalities for stress fractures: PubMed
- PET-MRI in stress fractures of the foot — PMC/NIH: PMC
- Stress fractures in primary care — BMJ / BJSM: PMC
- LSHTM modelling study — additional cancer deaths due to diagnostic delay: LSHTM
- UK Cancer Delayed Diagnosis Death Risk 2025: WeCovr
Dr Prashant Sankaye FRCR is a Consultant Musculoskeletal, Spine and Sports Radiologist and the lead radiologist at LSRI (London Sports and Rheumatology Imaging). He has almost three decades of medical experience, including a prestigious fellowship at Oxford University Hospitals, and specialises in sports injuries, bone stress pathology, spinal imaging and rheumatological conditions. He is the founder of Scannearme, a UK-wide network providing affordable, expert-reported MRI scans without the need for hospital referral. Dr Sankaye is a passionate advocate for early, accurate diagnosis and patient safety, and believes that “diagnose first, treat later” should be the guiding principle in all musculoskeletal and inflammatory disease management. For more information on diagnostic standards, visit the Royal College of Radiologists.
About the Author: Dr Prashant Sankaye, Consultant Musculoskeletal specialist and Radiologist, MBBS, MS, FCPS, MRCS, CCBST, FRCR, PGCE(Med), FHEA, PGDip Sports and Exercise Medicine
Dr Prashant Sankaye is a highly respected Consultant MSK Radiologist and the Clinical Director of London Sports & Rheumatology Imaging (LSRI). With over a decade of sub-specialty experience, he is a recognized expert in advanced diagnostic imaging (Ultrasound & 3T MRI) and precision ultrasound-guided therapeutic injections. His authoritative approach ensures patients avoid surgery where possible and receive the highest standard of orthopaedic, rheumatological, and sports medicine care.