✍️ Written by: LSRI Editorial Team
🩺 Medically Reviewed by: Dr Prashant Sankaye, Consultant Musculoskeletal specialist and Radiologist, MBBS, MS, FCPS, MRCS, CCBST, FRCR, PGCE(Med), FHEA, PGDip Sports and Exercise Medicine
📅 Last Updated: May 4, 2026
⏱️ Read Time: 7 Minutes
Avascular necrosis hip rehabilitation requires expert diagnosis and management.
This is a clinically important question, and the answer is that early-stage (Stage 1–2) AVN rehabilitation must prioritise joint offloading and muscle activation rather than aggressive loading. Here is the evidence-based exercise framework:
The Golden Rule: Protect the Femoral Head
The entire early rehab programme is built around one principle — reduce compressive load on the necrotic femoral head while maintaining muscle function and joint mobility. High-impact, weight-bearing exercises are contraindicated until orthopaedic and imaging review confirms the articular surface is stable.
Phase 1 — Isometric & Non-Weight Bearing (Weeks 1–6)
These are the safest exercises for Stage 1–2 AVN. Muscles contract without joint movement, preserving strength without stressing the femoral head.
- Isometric hip abduction — lying supine, press leg outward against a wall or theraband, hold 5–10 seconds, 3 sets of 10
- Isometric glute squeeze — lying supine, contract buttocks and hold, 10 repetitions
- Supine heel slides — lying flat, slowly slide heel toward buttocks and back, 10 reps twice daily — gentle hip flexion ROM without load
- Supine hip abduction on slider — lying on back, slide leg outward slowly, 10 reps, 2 sets
- Seated heel raises / toe raises — seated in chair, raise heels then toes alternately — activates calf and tibialis without hip compression
- Ankle pumps — essential for venous return and reducing intraosseous pressure in the femoral head
Phase 2 — Gentle Strengthening (Weeks 6–12, if stable on MRI)
Progress only if pain is not worsening and imaging review is favourable.
- Supine glute bridges — feet flat, lift hips to form a straight line, squeeze glutes, lower slowly; 3 sets of 15 — activates glute max and reduces hip flexor dominance
- Banded glute med bridges — theraband above knees during bridge to activate gluteus medius, which is critical for reducing lateral hip joint reaction forces
- Clam shells — sidelying with knees bent, rotate top knee upward; 3 sets of 15 — isolates gluteus medius without axial load
- Standing hip flexion (AROM) — holding chair, gently lift knee to hip height; 10 reps, 3 sets
- Standing hip extension — holding chair, leg straight behind, controlled movement; 10 reps, 3 sets
- Seated hamstring stretch — hold 20 seconds, 3 repetitions — maintains posterior chain flexibility
Phase 2 — Cardiovascular Fitness (Low-Impact)
Maintaining cardiovascular fitness and healthy weight reduces mechanical load on the hip throughout rehabilitation.
- Stationary cycling — the single best cardio option; non-weight bearing through the hip, low compressive force, can be started early
- Hydrotherapy / pool walking — water buoyancy reduces effective body weight on the femoral head by up to 50–75%; also improves range of motion and reduces pain
- Swimming — freestyle and backstroke are appropriate; avoid breaststroke (wide hip abduction under load)
Phase 3 — Functional Strengthening (3–6 months, guided by imaging)
Only progress to these if MRI confirms no articular collapse:
- Bilateral squats with theraband — controlled depth, weight distributed evenly
- Step-ups — low step height initially, progress carefully
- Single-leg balance — progressing proprioception for gait stability
- Gait re-training — with physiotherapist, correcting Trendelenburg pattern caused by weak gluteus medius
What to Avoid Completely
- Running, jumping, or high-impact sport
- Single-leg standing exercises in early phases
- Deep squats or lunges with full body weight
- Breaststroke swimming
- Any exercise causing groin or anterior hip pain during or after
Key Supporting Evidence
A multicentre study published in BMJ Open Sport & Exercise Medicine found that patients who completed a structured exercise programme after core decompression delayed the need for hip replacement by 3 years compared to those who had surgery alone. Even in conservatively managed Stage 1–2 AVN, therapeutic exercise that preserves hip muscle function and joint mobility is strongly supported.
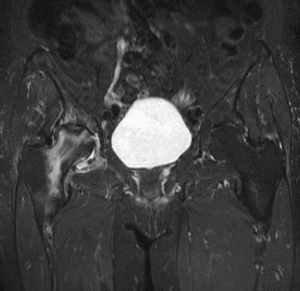
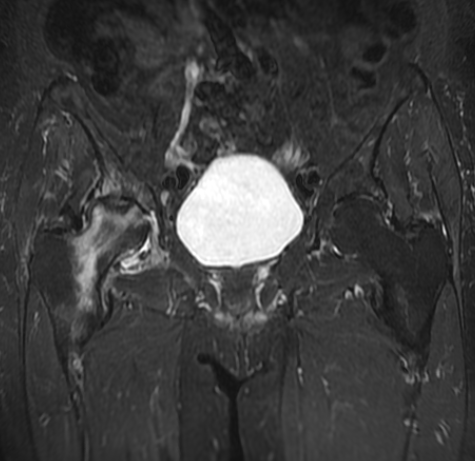
Important clinical note: As the MRI images you shared demonstrate established AVN with secondary OA, any rehabilitation programme should be guided by a musculoskeletal physiotherapist working alongside your imaging findings. The programme above applies to early-stage disease — patients with articular collapse (Stage 3–4) require orthopaedic co-management before progressing any loading exercise.
Dr Prashant Sankaye is a specialist musculoskeletal radiologist and CPD Approved Trainer at London Sports and Rheumatology Imaging (LSRI Ltd), CPD Provider #790052. ![]()
Understanding the Stages of Avascular Necrosis and Their Impact on Exercise
Exercise prescription for avascular necrosis (AVN) must be stage-appropriate. The internationally accepted Steinberg classification defines AVN progression from Stage 0 (preclinical) to Stage VI (severe joint collapse and secondary arthritis). Exercise tolerance and rehabilitation goals differ substantially across these stages.
- Stage I–II (Early): Bone marrow oedema and early sclerosis on MRI. No collapse. Conservative rehabilitation is appropriate. Focus on non-weight bearing strengthening and joint mobility.
- Stage III (Pre-collapse): Crescent sign visible on MRI — the subchondral bone is at risk. Protected weight bearing with crutches. Aquatic therapy is the mainstay of exercise.
- Stage IV–V (Collapse): Femoral head collapse with progressive joint space narrowing. Surgical options (core decompression, total hip replacement) are typically discussed. Gentle hydrotherapy may continue.
- Stage VI: End-stage arthritis. Surgical management is usually indicated.
Accurate staging requires MRI. At LSRI, Dr Prashant Sankaye provides detailed AVN staging reports to guide the treating orthopaedic and physiotherapy teams. Research from PubMed (Journal of Bone and Joint Surgery) confirms MRI as the most sensitive modality for early-stage AVN detection and staging.
The Role of the Physiotherapist in AVN Rehabilitation
Physiotherapy-led rehabilitation is central to managing AVN conservatively. An experienced musculoskeletal physiotherapist will design a programme incorporating:
- Hip abductor strengthening (gluteus medius) to offload the femoral head during any weight-bearing activities
- Hip flexor and extensor strengthening in non-weight bearing positions (lying and seated)
- Core stabilisation exercises to reduce compensatory lumbar loading
- Gait retraining with appropriate walking aid to minimise joint reaction forces
- Proprioception and balance training as tolerated
Monitoring Progress: Serial MRI in AVN Rehabilitation
One of the most important aspects of AVN management is monitoring for progression or improvement. Serial MRI scans at 3–6 month intervals allow the clinical team to:
- Assess whether bone marrow oedema is resolving (a positive prognostic sign)
- Detect early subchondral collapse before it becomes irreversible
- Confirm stability before advancing rehabilitation intensity
- Guide the decision between continued conservative management and surgical intervention
Frequently Asked Questions About AVN Hip Rehabilitation
Can AVN heal without surgery?
Early-stage AVN (Stage I–II) has the best potential for conservative management. Some patients achieve stabilisation or partial resolution with protected weight bearing, targeted rehabilitation, and addressing underlying causes (e.g. stopping corticosteroids, treating alcohol dependency). However, more advanced stages typically require surgical intervention.
How long does AVN rehabilitation take?
The timeline varies enormously based on stage at diagnosis and individual response. Early-stage patients may rehabilitate over 3–6 months. Those awaiting or recovering from total hip replacement require a longer programme of 6–12 months.
Should I stop all exercise with AVN?
No. Inactivity leads to muscle atrophy, reduced cardiovascular fitness, and worsening quality of life. The goal is to find appropriate, joint-protective exercise. Aquatic exercise and stationary cycling are almost universally recommended at all stages.
If you have been diagnosed with avascular necrosis or hip pain and require expert MRI assessment, contact LSRI to arrange an appointment with Dr Prashant Sankaye. For further clinical reading on AVN, the NHS information on avascular necrosis provides a helpful overview.
Avascular Necrosis Hip Rehabilitation – Summary
Understanding avascular necrosis hip rehabilitation is crucial for optimal recovery.
Essential Tips for Avascular Necrosis Hip Rehabilitation
Effective avascular necrosis hip rehabilitation starts slowly.
Commit to your avascular necrosis hip rehabilitation program.
Supervised avascular necrosis hip rehabilitation yields the best results.
Your avascular necrosis hip rehabilitation journey requires patience.
Discover the ideal avascular necrosis hip rehabilitation strategies.
Avascular necrosis hip rehabilitation focuses on offloading the joint.
About the Author: Dr Prashant Sankaye, Consultant Musculoskeletal specialist and Radiologist, MBBS, MS, FCPS, MRCS, CCBST, FRCR, PGCE(Med), FHEA, PGDip Sports and Exercise Medicine
Dr Prashant Sankaye is a highly respected Consultant MSK Radiologist and the Clinical Director of London Sports & Rheumatology Imaging (LSRI). With over a decade of sub-specialty experience, he is a recognized expert in advanced diagnostic imaging (Ultrasound & 3T MRI) and precision ultrasound-guided therapeutic injections. His authoritative approach ensures patients avoid surgery where possible and receive the highest standard of orthopaedic, rheumatological, and sports medicine care.