✍️ Written by: LSRI Editorial Team
🩺 Medically Reviewed by: Dr Prashant Sankaye, Consultant Musculoskeletal specialist and Radiologist, MBBS, MS, FCPS, MRCS, CCBST, FRCR, PGCE(Med), FHEA, PGDip Sports and Exercise Medicine
📅 Last Updated: May 4, 2026
⏱️ Read Time: 7 Minutes
Osteonecrosis hip mri diagnosis london requires expert diagnosis and management.
If you have had hip pain for three months or more and been told it is “just wear and tear” or early arthritis, this post is for you. As a specialist in sports and rheumatology imaging, I regularly see patients who have been living with avascular necrosis (AVN) of the hip — also called osteonecrosis — that was missed or delayed in diagnosis. The consequences of that delay can be permanent and irreversible.
This article explains what osteonecrosis is, why it looks different from ordinary osteoarthritis on MRI, and why early, expert imaging is the single most important step you can take to protect your hip joint.
What Is Avascular Necrosis (Osteonecrosis) of the Hip?
Avascular necrosis (AVN), or osteonecrosis, is the death of bone tissue caused by a disrupted blood supply to the femoral head — the ball part of your hip joint. Without adequate blood flow, the bone cells die, the femoral head weakens, and eventually the joint surface collapses.
Unlike osteoarthritis, which is a gradual wearing of cartilage over many years, AVN can destroy a hip joint relatively quickly — often within months to a couple of years if not identified and managed early.
Key fact: AVN can be completely invisible on a plain X-ray in its early, treatable stages. MRI is the gold standard for diagnosis.
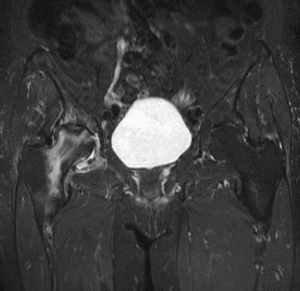
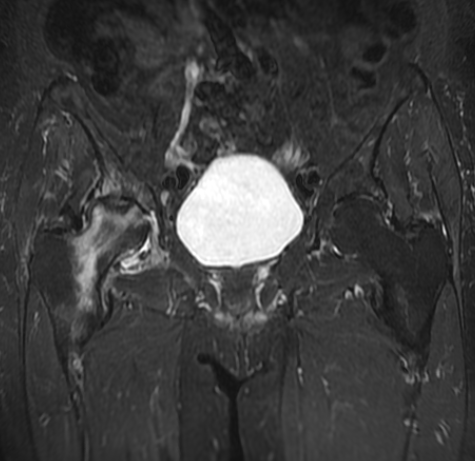
The MRI You See Above — What Does It Show?
(Image: MRI hip – Dr Prashant Sankaye, London Sports and Rheumatology Imaging)
The MRI images in this post show exactly what I see in clinical practice. This is a multiplanar MRI of the hip, with coronal T2 STIR, coronal T1, sagittal and axial sequences. Together, they tell a very specific story:
- Coronal T2 STIR (top left): The bright signal in the femoral head indicates bone marrow oedema — a hallmark of early to established AVN. The “double-line sign,” a classic MRI feature of osteonecrosis, may be present.
- Coronal T1 (top right): Low signal within the femoral head confirms the zone of ischaemic necrosis — dead bone. This is the definitive finding.
- Sagittal and axial views (bottom): These confirm the extent of involvement, whether the articular surface is at risk of collapse, and whether secondary osteoarthritic changes are beginning.
This is no longer early-stage disease — the scan shows established AVN that has progressed to secondary osteoarthritis (OA). This is precisely why timely diagnosis matters so much.
Why Is AVN So Often Missed?
In my experience, there are several common reasons:
- Symptoms mimic other conditions — groin pain, thigh pain, and restricted hip movement are common to many diagnoses including labral tears, hip impingement (FAI), and tendinopathy
- X-rays appear normal in early stages — stage 1 AVN is completely invisible on X-ray
- It affects a younger population — patients in their 30s and 40s are often not immediately suspected of having joint-threatening pathology
- Risk factors are not always obvious — steroid use, alcohol, blood clotting disorders, and previous trauma are known triggers, but many cases are idiopathic
The Stages of Hip Osteonecrosis
Understanding the stages helps explain why urgency matters. We use clinical staging systems (like the ARCO classification) to guide treatment:
| Stage | What’s Happening | X-ray | MRI |
|---|---|---|---|
| Stage 1 | Dead bone, no collapse | Normal | Abnormal ✅ |
| Stage 2 | Bone changes visible | Abnormal | Abnormal |
| Stage 3 | Crescent sign — collapse beginning | Crescent sign | Collapse visible |
| Stage 4 | Femoral head collapsed + OA | Collapse + OA | Advanced changes |
Stages 1 and 2 are the window of opportunity for joint-preserving treatment. By Stage 3–4, the options become significantly more limited — and hip replacement becomes increasingly likely.
Why MRI Is the Only Test That Catches It in Time
MRI is the most sensitive imaging test for diagnosing AVN — significantly more sensitive than X-ray, CT, or bone scan in the early stages. At London Sports and Rheumatology Imaging, we use high-quality, dedicated musculoskeletal MRI protocols that are specifically optimised for the hip, covering:
- T1-weighted sequences — to identify the zone of necrosis
- T2 STIR sequences — to detect bone marrow oedema and inflammatory changes
- Sagittal and axial planes — to assess the full extent of disease and articular surface integrity
This is not a standard “hip MRI” — it is a specialist, clinically guided examination interpreted by a musculoskeletal radiologist with expertise in exactly this type of pathology.
Who Is at Risk of AVN of the Hip?
You should seek expert hip MRI imaging if you have hip pain and any of the following:
- Long-term or high-dose corticosteroid use (e.g. for asthma, IBD, rheumatological conditions)
- Excessive alcohol consumption
- Previous hip trauma or dislocation
- Sickle cell disease or other haematological conditions
- Systemic lupus erythematosus (SLE) or other connective tissue diseases
- Unexplained hip or groin pain lasting more than 4–6 weeks with no clear diagnosis
- Previous COVID-19 infection (emerging evidence links prolonged steroid use in COVID treatment to AVN)
What Happens After Diagnosis?
Early-stage AVN (Stages 1–2) offers real treatment options:
- Core decompression — surgical procedure to restore blood flow and reduce pressure in the femoral head
- Bone marrow concentrate / regenerative therapy — newer evidence-based approaches
- Protected weight-bearing and physiotherapy — to reduce load on the at-risk femoral head
- Bisphosphonate therapy — may slow bone loss in selected cases
- Close monitoring — repeat MRI at intervals to track progression
Late-stage disease (Stages 3–4, as seen in the MRI images above) with established osteoarthritis typically requires orthopaedic surgical review and often hip replacement.
The critical point: the earlier the diagnosis, the more choices you have.
Why Choose London Sports and Rheumatology Imaging?
At London Sports and Rheumatology Imaging, we combine specialist expertise with high-resolution musculoskeletal MRI to deliver diagnoses that make a real clinical difference.
- Dr Prashant Sankaye is a specialist in sports and rheumatology imaging with extensive experience in hip pathology
- We are a CPD Approved Provider (#790052) — independently accredited by The CPD Group, reflecting our commitment to clinical excellence
- Our reports are detailed, clinically relevant, and actionable — giving you and your referring clinician a clear pathway forward
- We work with patients, GPs, physiotherapists, rheumatologists, and orthopaedic surgeons across London
“Don’t wait three more months. If your hip pain hasn’t been properly explained, the answer may be in the MRI.”
— Dr Prashant Sankaye
Book a Specialist Hip MRI
If you or your patient has unexplained hip pain, do not wait for an X-ray to become abnormal. Contact London Sports and Rheumatology Imaging to discuss a specialist hip MRI.
📞 0203 633 5040
🔗 Book Online
📍 London
Dr Prashant Sankaye is a specialist musculoskeletal radiologist and CPD Approved Trainer at London Sports and Rheumatology Imaging (LSRI Ltd), CPD Provider #790052. ![]()
Frequently Asked Questions About Hip AVN and MRI
Is AVN always caused by steroid use?
No. While corticosteroid use and excessive alcohol consumption are the most common identifiable causes, approximately 20–30% of AVN cases are idiopathic (no identifiable cause). Other causes include trauma, sickle cell disease, systemic lupus erythematosus, and hyperbaric exposure.
How quickly does AVN progress?
Disease progression is highly variable. Some early-stage patients remain stable for years; others progress to femoral head collapse within months. This unpredictability is why regular serial MRI monitoring is essential.
Is hip AVN the same in both hips?
AVN is bilateral in approximately 40–80% of cases when caused by corticosteroids or alcohol. It is essential that both hips are imaged when AVN is diagnosed in one hip.
What treatments are available before total hip replacement?
Core decompression (drilling to relieve pressure and stimulate healing), bone grafting, and osteotomy are surgical options for early-stage AVN. PRP injections and bisphosphonate therapy have been investigated as adjuncts. Total hip replacement is reserved for later-stage disease with femoral head collapse.
For comprehensive NHS guidance on avascular necrosis, visit the NHS AVN information page. For detailed clinical staging information, Radiopaedia’s AVN article is an excellent reference used by radiologists and clinicians worldwide.
If you suspect AVN or have been told you may have this condition, contact LSRI today for a rapid-access MRI assessment. Early diagnosis is the single most important factor in preserving your hip joint.
Osteonecrosis Hip Mri Diagnosis London – Summary
Understanding osteonecrosis hip mri diagnosis london is crucial for optimal recovery.
Essential Tips for Osteonecrosis Hip Mri Diagnosis London
Early osteonecrosis hip mri diagnosis london is critical.
Our osteonecrosis hip mri diagnosis london specialists can help.
Choose the best osteonecrosis hip mri diagnosis london clinic.
Without osteonecrosis hip mri diagnosis london, treatment is delayed.
An accurate osteonecrosis hip mri diagnosis london makes all the difference.
About the Author: Dr Prashant Sankaye, Consultant Musculoskeletal specialist and Radiologist, MBBS, MS, FCPS, MRCS, CCBST, FRCR, PGCE(Med), FHEA, PGDip Sports and Exercise Medicine
Dr Prashant Sankaye is a highly respected Consultant MSK Radiologist and the Clinical Director of London Sports & Rheumatology Imaging (LSRI). With over a decade of sub-specialty experience, he is a recognized expert in advanced diagnostic imaging (Ultrasound & 3T MRI) and precision ultrasound-guided therapeutic injections. His authoritative approach ensures patients avoid surgery where possible and receive the highest standard of orthopaedic, rheumatological, and sports medicine care.