✍️ Written by: LSRI Editorial Team
🩺 Medically Reviewed by: Dr Prashant Sankaye, Consultant Musculoskeletal specialist and Radiologist, MBBS, MS, FCPS, MRCS, CCBST, FRCR, PGCE(Med), FHEA, PGDip Sports and Exercise Medicine
📅 Last Updated: May 4, 2026
⏱️ Read Time: 6 Minutes
Hydrotherapy avascular necrosis hip requires expert diagnosis and management.
Both hydrotherapy and stationary cycling are considered first-line conservative interventions for avascular necrosis (AVN) rehabilitation. They achieve the cardinal goal: maintaining fitness, strength, and mobility without compressing the vulnerable femoral head.
Why Offloading Is Everything in AVN
The necrotic femoral head is mechanically weakened and at risk of subchondral collapse under axial load. Every rehabilitation decision in early-stage AVN is filtered through one question: does this exercise put compressive force through the femoral head?
Both hydrotherapy and stationary cycling pass that test — which is why they sit at the top of the AVN rehab hierarchy.
Hydrotherapy in AVN Recovery
Water buoyancy reduces effective body weight transmitted through the hip joint by up to 75% when immersed to chest depth, allowing movement and muscle activation that would be impossible or harmful on land. This makes hydrotherapy the single most versatile rehabilitation environment for AVN patients.
Physiological Benefits
- Buoyancy directly reduces joint compressive load — at chest depth, only ~25% of body weight passes through the hip
- Hydrostatic pressure (water pressing uniformly against the body) reduces swelling, improves venous return, and — critically in AVN — may help reduce elevated intraosseous pressure in the femoral head, which is a key driver of ischaemia
- Warm water (34°C) promotes muscle relaxation, reduces pain, and increases tissue extensibility, improving range of motion without stress
- Water resistance provides gentle, graded strengthening of hip abductors and extensors in all planes simultaneously
Evidence
A study of 192 patients with hip OA and post-THR found that those who completed water-based rehabilitation showed significantly greater reductions in pain (p<0.001), greater range of motion gains, and significantly reduced NSAID use compared to land-based exercise alone. For AVN specifically, a leading London sports medicine clinic uses pool-based rehabilitation 3–4 times per week as the exclusive exercise modality for the first 8 weeks, with no land-based exercise permitted during that phase.
Practical Hydrotherapy Protocol for AVN
| Exercise | Depth | Sets/Reps | Notes |
|---|---|---|---|
| Pool walking forward/backward | Chest | 10 min continuous | Begin at week 1 |
| Standing hip abduction in water | Waist–chest | 3 × 15 each leg | Slow, controlled |
| Standing hip extension | Waist | 3 × 15 | Hold pool rail |
| Water treading / flutter kick | Horizontal | 5–10 min | No breaststroke |
| Aqua jogging with belt | Chest | 10–15 min | Weeks 4–8 onward |
| Hip circles | Chest | 2 × 10 each direction | Pain-free range only |
Stationary Cycling in AVN Recovery
Stationary cycling is the best land-based cardiovascular option for AVN because the pedalling motion is predominantly rotational rather than axial — meaning the force goes around the joint rather than compressing down through it. Even patients who cannot complete full pedal revolutions can benefit from partial arc cycling (rocking the pedals back and forth), which maintains joint lubrication and gentle ROM.
Why It Works
- Non-weight bearing through the hip — the saddle supports body weight, not the femoral head
- Rhythmic motion promotes synovial fluid circulation, which nourishes articular cartilage even where blood supply is compromised
- Quadriceps and glute activation without hip joint impingement — essential for maintaining muscle bulk and preventing Trendelenburg gait
- Cardiovascular fitness is maintained, which supports bone healing and reduces the metabolic impact of reduced activity
- Weight management — if elevated BMI contributed to AVN onset or progression, cycling provides caloric expenditure without joint penalty. Aquatic therapy in obese patients (BMI >30) improves hip ROM by 20–30% without exacerbating pain.
Practical Cycling Protocol for AVN
| Phase | Duration | Resistance | Cadence | Notes |
|---|---|---|---|---|
| Week 1–2 | 10 min/day | Zero (0) | Comfortable | Partial arc if full rotation painful |
| Week 3–4 | 15–20 min/day | Very light | 60–70 rpm | Full rotation if tolerated |
| Week 5–8 | 20–30 min/day | Light | 70–80 rpm | Twice daily if tolerated |
| Week 8+ | 30–45 min/day | Moderate | 80–90 rpm | Only if MRI review confirms stability |
Saddle height is critical — set high enough that the knee is almost fully extended at the bottom of the pedal stroke, minimising hip flexion range and compressive load at end-range.
Combined Protocol: The Evidence-Based Approach
The strongest outcomes in AVN conservative management come from combining both modalities. A suggested weekly structure for early-stage AVN:
- Mon / Wed / Fri — Hydrotherapy (30–45 mins, pool-based exercises)
- Tue / Thu / Sat — Stationary cycling (20–30 mins, zero to low resistance)
- Daily — Isometric hip exercises (supine, non-weight bearing)
- All days — Crutch-assisted ambulation to minimise walking load on the femoral head
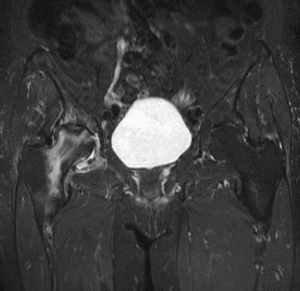
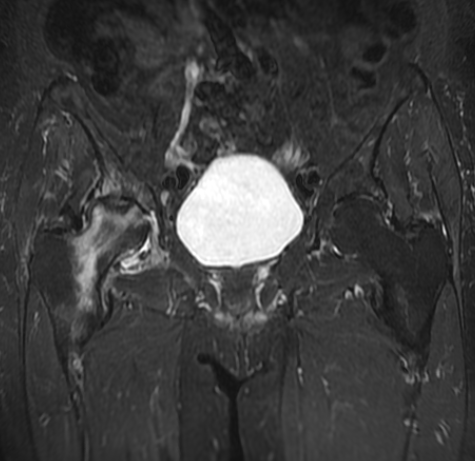
Important Caveat: As the MRI images discussed previously demonstrate established AVN with secondary osteoarthritis (Stage 3–4 changes), both hydrotherapy and cycling remain appropriate but the overall programme must be coordinated with orthopaedic review. The goal at that stage shifts from joint preservation to pain management, function maintenance, and surgical planning — and both modalities remain the safest way to keep the patient active while that pathway is determined.
Dr Prashant Sankaye is a specialist musculoskeletal radiologist and CPD Approved Trainer at London Sports and Rheumatology Imaging (LSRI Ltd), CPD Provider #790052. ![]()
The Evidence Base for Hydrotherapy in AVN
Aquatic rehabilitation for hip conditions, including avascular necrosis, is well-supported by clinical evidence. Water immersion to chest depth reduces the effective body weight transmitted through the hip joint by approximately 80%. This dramatic reduction in joint loading allows patients to exercise at intensities that would be impossible on land, maintaining cardiovascular fitness and muscle strength without accelerating bone collapse.
Research published on PubMed confirms that aquatic exercise programmes improve pain, function, and quality of life in patients with hip joint pathology, with an excellent safety profile.
Structuring a Hydrotherapy Programme for AVN
A well-structured hydrotherapy programme for AVN typically progresses through three phases:
Phase 1 (Weeks 1–4): Establishing Tolerance
- Water walking at chest depth — forward, backward, and sideways
- Stationary cycling in the water using a pool bike (zero impact)
- Gentle range of motion exercises: hip flexion and extension, abduction and adduction
- Duration: 20–30 minutes, 3 times per week
Phase 2 (Weeks 5–10): Building Strength
- Progressive resistance using water resistance gloves and ankle floats
- Single-leg balance in shallow water (limited weight bearing as appropriate for stage)
- Hip abductor strengthening against water resistance
- Duration: 30–40 minutes, 3–4 times per week
Phase 3 (Weeks 10+): Functional Progression
- Gradual transition to shallow water walking to reintroduce partial weight bearing
- Coordination with land-based physiotherapy as tolerated
- Cardiovascular interval training in the pool
Stationary Cycling: The Perfect Land-Based Complement
When pool access is unavailable, a properly adjusted stationary cycle provides an excellent alternative. Key adjustments for AVN patients include:
- Seat height set high enough that the knee reaches only partial flexion (reducing hip joint contact forces)
- Resistance set low — the goal is circulation and muscle activation, not cardiovascular stress testing
- Upright posture to avoid excessive hip flexion
- Duration of 15–30 minutes at comfortable cadence, building gradually
Monitoring Your AVN with Serial MRI
It is essential that patients undertaking conservative rehabilitation for AVN have regular imaging follow-up. At LSRI, we recommend serial MRI at 3–6 month intervals to confirm that bone marrow oedema is resolving and that the femoral head remains structurally intact. Any change in pain pattern or new onset of groin/hip pain should prompt an early review and urgent MRI.
For further information on aquatic rehabilitation, the NHS physiotherapy guidance outlines how specialist physiotherapy can support recovery from musculoskeletal conditions. Contact LSRI to discuss your AVN MRI assessment and rehabilitation planning.
Hydrotherapy Avascular Necrosis Hip – Summary
Understanding hydrotherapy avascular necrosis hip is crucial for optimal recovery.
Essential Tips for Hydrotherapy Avascular Necrosis Hip
The role of hydrotherapy avascular necrosis hip recovery is huge.
Safe hydrotherapy avascular necrosis hip programs are available.
Enjoy hydrotherapy avascular necrosis hip sessions safely.
Optimise your hydrotherapy avascular necrosis hip outcomes.
Expert hydrotherapy avascular necrosis hip guidance matters.
About the Author: Dr Prashant Sankaye, Consultant Musculoskeletal specialist and Radiologist, MBBS, MS, FCPS, MRCS, CCBST, FRCR, PGCE(Med), FHEA, PGDip Sports and Exercise Medicine
Dr Prashant Sankaye is a highly respected Consultant MSK Radiologist and the Clinical Director of London Sports & Rheumatology Imaging (LSRI). With over a decade of sub-specialty experience, he is a recognized expert in advanced diagnostic imaging (Ultrasound & 3T MRI) and precision ultrasound-guided therapeutic injections. His authoritative approach ensures patients avoid surgery where possible and receive the highest standard of orthopaedic, rheumatological, and sports medicine care.